Abstract
Background: Maternity continuum of care is the continuity of maternal health care services given to mothers during antenatal period, child birth and post natal period. It is one of the strategic programs meant to lower the death rates of mothers, newborns, and children. In spite of this, a large number of moms discontinue their participation in maternal continuum care. Dropout from the maternity continuum of care is prevalent public health issue in underdeveloped nations, such as Ethiopia. Methods: Community based quantitative cross-sectional study was carried out among 357 mothers who gave birth in the 12 months in Adigrat town. Systematic sampling method was used to obtain study participants. Data was collected using pretested, semi- structured and face to face interviewer administered questioner. Bivariable and multivariable logistic regression model was fitted. Variables having p-value less than 0.2 in bivariable analysis was entered to multivariable logistic regression model. In multivariable logistic regression adjusted odds ratio with 95% confidence interval was used to determine strength and direction of the association between dependent and independent variables. Results: The overall magnitude of drop out from the maternity continuum of care was 237 (66.4%) [95%CI (61.3-70.9)], 60.6% drop out from ANC visit, 5.6% drop out from skill birth attendant and 58.9% drop out from PNC. Mothers never heard on maternal health care service (AOR=4.179 (1.107, 15.783), service out of health facility (AOR =5.136 (1.988, 13.267) noabortionhistory (AOR=1.424 (1.113, 12.133), unplannedpregnancy (AOR=5.478 (1.902, 15.777), less than 4 ANC visit (AOR= 5.583 (2.598, 11. 997) and mothers attitude (AOR=15.049 (2.489, 32.997) were statically significant factors associated with drop out from maternity continuum of care. Conclusion and discussion: This study showed that magnitude of drop out from maternity continuum of care was high as compared to WHO recommendations. As a result concerned stakeholders and policy makers should initiate more than four ANC visit, create awareness on harmful traditional practice, bad pregnancy history, support mothers to use family planning to prevent unplanned pregnancy, and work on attitude change of the community.
|
Published in
|
American Journal of Life Sciences (Volume 12, Issue 6)
|
|
DOI
|
10.11648/j.ajls.20241206.13
|
|
Page(s)
|
121-133 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2024. Published by Science Publishing Group
|
Keywords
Drop out, Maternity Connituunm of Care, Associated Factors, After War, Adigrat Tow
1. Introduction
Maternity continuum of care is defined as the continuity of maternal health care services provided to mothers during antenatal period (ANC), child birth and post natal period (PNC)
| [1] | Owili PO, Muga MA, Mendez BR, Chen B. Quality of maternity care and its determinants along the continuum in Kenya: A structural equation modeling analysis. PloS one. 2017; 12(5): e0177756. |
[1]
. It is one of the strategic plans that has been developed to reduce half million of maternal deaths, 4 million neonatal deaths, and 6 million child deaths in one year and to improve maternal and neonatal wellbeing. This integrated services that address the entire continuum from the antepartum to the postnatal period are important for gains in maternal and child survival and to reduce complications for both the mother and her neonate
| [2] | Kerber KJ, de Graft-Johnson JE, Bhutta ZA, Okong P, Starrs A, Lawn JE. Continuum of care for maternal, newborn, and child health: from slogan to service delivery. The Lancet. 2007; 370(9595): 1358-69. |
| [3] | Agarwal S, Curtis S, Angeles G, Speizer I, Singh K, Thomas J. Are community health workers effective in retaining women in the maternity care continuum? Evidence from India. BMJ Global Health. 2019; 4(4): e001557. |
[2, 3]
. Despite of this advantage of many mothers they dropped out from maternity continuum of care. Maternity continuum of care should focus on quality of care because it is important not only to mothers but also their child
| [1] | Owili PO, Muga MA, Mendez BR, Chen B. Quality of maternity care and its determinants along the continuum in Kenya: A structural equation modeling analysis. PloS one. 2017; 12(5): e0177756. |
[1]
. Dropout of from maternity Continuum of care is considered as among women’s who received at least one ANC visit but did not receive skilled delivery assistants, and from those who got skilled birth attendants but did not receive at least one postnatal care within six weeks postpartum period in addition to the first 24 hours after institutional delivery
| [4] | Akinyemi JO, Afolabi RF, Awolude OA. Patterns and determinants of dropout from maternity care continuum in Nigeria. BMC pregnancy and childbirth. 2016; 16(1): 282. |
| [5] | Tamang TM, editor Factors associated with completion of continuum of Care for Maternal Health in Nepal. proceedings of the IUSSP XXVIII International Population Conference, Cape Town, South Africa; 2017. |
[4, 5]
.
According to World Health Organization (WHO) 2015 estimation worldwide approximately 303,000 maternal deaths are occur during labor, delivery and immediate postpartum period and majority of the death occurred in developing country, it accounts around 66% in Sub-Saharan Africa and 22% in Southern Asia
| [6] | Organization WH. World health statistics 2015: World Health Organization; 2015. |
| [7] | Alkema L, Chou D, Hogan D, Zhang S, Moller A-B, Gemmill A, et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. The Lancet. 2016; 387(10017): 462-74. |
[6, 7]
. The most common causes of maternal mortality that occurred during pregnancy and child birth complications are avoidable by providing proper care during pregnancy, delivery and postpartum period
| [8] | Singh K, Story WT, Moran AC. Assessing the continuum of care pathway for maternal health in South Asia and sub-Saharan Africa. Maternal and child health journal. 2016; 20(2): 281-9. |
[8]
however, many mothers in majority countries do not got ANC, skilled delivery care and PNC and also they dropped out from maternity continuum of care
| [9] | Anastasi E, Borchert M, Campbell OM, Sondorp E, Kaducu F, Hill O, et al. Losing women along the path to safe motherhood: why is there such a gap between women’s use of antenatal care and skilled birth attendance? A mixed methods study in northern Uganda. BMC pregnancy and childbirth. 2015; 15(1): 287. |
[9]
. Globally data showed that around 80% of maternal deaths could be prevented if women had access to essential maternity and basic health-care services during their pregnancy, child birth and postnatal period
| [10] | Landers C. Maternal and newborn health: a global challenge. The State of the World's Children New York, NY: United Nations Children's Fund. 2009; 5. |
[10]
. In South Asia and Sub –Saharan Africa the major drop-out more than 50% occurs early in the continuum of care between the first ANC visit and four ANC visits and more between pregnancy and delivery than between delivery and the postnatal period since having four ANC visits and receiving better quality of ANC affected women’s subsequent use of Skilled birth attendant (SBA)
| [5] | Tamang TM, editor Factors associated with completion of continuum of Care for Maternal Health in Nepal. proceedings of the IUSSP XXVIII International Population Conference, Cape Town, South Africa; 2017. |
| [8] | Singh K, Story WT, Moran AC. Assessing the continuum of care pathway for maternal health in South Asia and sub-Saharan Africa. Maternal and child health journal. 2016; 20(2): 281-9. |
[5, 8]
. Drop out in maternity continuum of care is widespread in low resource setting country including Ethiopia mostly postpartum period is affected
| [11] | Mohan D, LeFevre AE, George A, Mpembeni R, Bazant E, Rusibamayila N, et al. Analysis of dropout across the continuum of maternal health care in Tanzania: findings from a cross-sectional household survey. Health policy and planning. 2017; 32(6): 791-9. |
[11]
. Compared to antenatal care and skilled attendance at birth, postnatal care has been largely neglected in safe motherhood programs. Postnatal care, especially within the first 48 hours after birth, is critical to the management of postpartum hemorrhage, an important cause of maternal deaths in developing countries since, more than 60 percent of maternal deaths occur in developing countries are happened during the first six weeks after delivery. In addition, postnatal care provides a chance to improve the adoption of healthy behaviors for mother and child
| [2] | Kerber KJ, de Graft-Johnson JE, Bhutta ZA, Okong P, Starrs A, Lawn JE. Continuum of care for maternal, newborn, and child health: from slogan to service delivery. The Lancet. 2007; 370(9595): 1358-69. |
| [11] | Mohan D, LeFevre AE, George A, Mpembeni R, Bazant E, Rusibamayila N, et al. Analysis of dropout across the continuum of maternal health care in Tanzania: findings from a cross-sectional household survey. Health policy and planning. 2017; 32(6): 791-9. |
| [12] | Wang W. Levels and trends in the use of maternal health services in developing countries: ICF Macro; 2011. |
| [13] | Kikuchi K, Yasuoka J, Nanishi K, Ahmed A, Nohara Y, Nishikitani M, et al. Postnatal care could be the key to improving the continuum of care in maternal and child health in Ratanakiri, Cambodia. PloS one. 2018; 13(6): e0198829. |
[2, 11-13]
. Only 47% of women had their first ANC visit in the first trimester in South Asia, and this proportion was even lower in Sub-Saharan Africa which is 24%
| [8] | Singh K, Story WT, Moran AC. Assessing the continuum of care pathway for maternal health in South Asia and sub-Saharan Africa. Maternal and child health journal. 2016; 20(2): 281-9. |
[8]
.
In Ethiopia, the most common maternal health care service they received were ANC visit according mini Ethiopian demographic health survey (EDHS) of 2019 (74%) of woman receive at least one ANC visit by SBA during their pregnancy time and 43% women were receive four and above ANC but, the utilizations of professional assisted delivery care and PNC is low which is 48% and 34% respectively
| [14] | Ethiopian Public Health Institute FMoH, Addis Ababa, Ethiopia, and The DHS Program, ICF, Rockville, Maryland, USA. Mini Demographic and Health Survey. 2019. |
[14]
. This indicate that there is drop out in maternity continuum of care and this may lead to poor maternal and child health.
Different studies showed that there are many factors that hindered the rate of maternity continuum of care like low or lack of formal education, poverty and healthcare access problems (distance to facility, have not exposure to media, unplanned pregnancy, having<4 ANC follow up, Sociodemographic factors and difficulty with getting money for treatment
| [4] | Akinyemi JO, Afolabi RF, Awolude OA. Patterns and determinants of dropout from maternity care continuum in Nigeria. BMC pregnancy and childbirth. 2016; 16(1): 282. |
| [8] | Singh K, Story WT, Moran AC. Assessing the continuum of care pathway for maternal health in South Asia and sub-Saharan Africa. Maternal and child health journal. 2016; 20(2): 281-9. |
| [11] | Mohan D, LeFevre AE, George A, Mpembeni R, Bazant E, Rusibamayila N, et al. Analysis of dropout across the continuum of maternal health care in Tanzania: findings from a cross-sectional household survey. Health policy and planning. 2017; 32(6): 791-9. |
| [15] | Muluneh AG, Kassa GM, Alemayehu GA, Merid MW. High dropout rate from maternity continuum of care after antenatal care booking and its associated factors among reproductive age women in Ethiopia, Evidence from Demographic and Health Survey 2016. PloS one. 2020; 15(6): e0234741. |
[4, 8, 11, 15]
.
Most literatures carried out in the glove and even in Ethiopia were utilization of maternity continuum of care, any of the three components of maternity continuum of care (antenatal, delivery and postnatal care) and their result shows both utilization and its dropout separately in the three components. Therefore, this study will aims to provide clear information on prevalence of dropout from maternity continuum of care and associated factors among mothers who gave birth in the last 12 months in Adigrat town and also there is scarcity of information on drop out maternity continuum of care and associated factors in Ethiopia, particularly in the study area.
2. Justifications of the Study
According to mini EDHS 2019 report, out of all women aged 15–49 years who had a live birth in the 5 years before the survey, 74% received at least one (ANC) and 48% had skilled delivery assistance, among women age 15-49 giving birth in the 2 years before the survey, 34% had a postnatal checkup
| [14] | Ethiopian Public Health Institute FMoH, Addis Ababa, Ethiopia, and The DHS Program, ICF, Rockville, Maryland, USA. Mini Demographic and Health Survey. 2019. |
[14]
. This indicates around 26% of those who received antenatal care mothers were dropped out before delivery, and almost 14% of those who received skilled delivery assistance dropped out before postnatal care. This drop out in continuity of care is one contributing factor for poor maternal, neonatal and child health outcomes.
Limited studies have been conducted on the prevalence of drop out from maternity continuum of care and its associated factor in the study area, even in major part of Ethiopia. Maternity continuum of care is strategic plan to reduce maternal and neonatal mortality therefore, identifying magnitude of dropout of continuum care will be important for government and health mangers to suggest interventions in improving maternal and neonatal health.
This study will also provide greater input to the government and program managers for proper implementation and evaluation of their contribution for the achievement of Sustainable Development Goals (SDGs) in which the third SDG aimed for improving the maternal, newborn and child health as primary concern
| [16] | EMOH. Ethiopia Voluntary National Review on SDGs Government Commitments, National Ownership and Performance Trends. 2017. |
[16]
.
Finally the finding of this study will be used as a bench mark for further researchers and stake holders to conduct intervention study in the study area as well as in the country.
3. Methods
3.1. Study Design and Period
Community based quantitative cross-sectional study was conducted from March 30-May 30/2024.
3.2. Study Area
This study was conducted in Adigrat town Tigray Ethiopia. Adigrat town is one of the zonal towns found in Eastern Tigray zone. It is located around 900 Km North of Addis Ababa, capital city of Ethiopia and 108 Km from Mekele, the capital city of Tigray Regional state. It has six kebeles (smallest administrative unit in Ethiopia), one general hospital, two health centers, two high schools and 4 elementary schools. According to 2007 national census conducted by the central statistical agency of Ethiopia (CSA), the town has a total population of 57,588; of those 26,010 are men and 31,578 women. The majority of the population Orthodox Christianity followers, with 94.01% while 3.02% of the populations were Catholics followers, and 2.68% were Muslim.
3.3. Population
3.3.1. Source Population
All mothers who gave birth in the last 12 months in Adigrat town.
3.3.2. Study Population
All mothers who gave birth in the last 12 months in Adigrat town in the selected kebeles.
3.3.3. Inclusion and Exclusion Criteria
(i). Inclusion Criteria
All mothers who gave birth in the last 12 months in Adigrat town who resides for 6 months prior the study and above in the town.
Mothers who had at least one antenatal care (ANC) visit during her pregnancy.
(ii). Exclusion Criteria
Women who eligible but, they are serious ill and unable to communicate effectively during data collection period will be excluded from the study.
3.4. Sample Size Estimation
The sample size was determined using single population proportion by assuming mothers who had at least one ANC visit drop out from maternity continuum of care 69.1%, from study conducted in DebreBrhane town
| [17] | Tadese M, Tessema SD, Aklilu D, Wake GE, Mulu GB. Dropout from a maternal and newborn continuum of care after antenatal care booking and its associated factors in Debre Berhan town, northeast Ethiopia. Frontiers in Medicine. 2022; 9: 950901. |
[17]
, with a 95% confidence level and 5% marginal error and 10% non-response rate. Based on these assumptions, the total sample size was calculated using the following formula:
Where n = required sample size, Z = critical value for normal distribution at 95% confidence level (1.96) P =prevalence of drop out from maternity continuum care d = 0.05 (5% margin of error), by considering 10% non-response rate of = 33 and, the minimum adequate sample size was found 361.
3.5. Sampling Procedure
Systematic sampling technique was used to obtain study participants. Adigrat town has 6 kebeles by lottery method three kebeles were selected. From each selected kebles we were take mothers who gave birth in the last 12 months by systematic method and had at least one ANC visit during her last pregnancy as a sample. The health extension workers were responsible for identifying households who gave birth in the last 12 months. We will be abstracted the lists of women’s who are eligible from the log book of health extension workers. Households having two mothers who gave birth in the last 12 months one mother was selected by lottery method.
3.6. Variables of the Study
3.6.1. Dependent Variable
Drop out from maternity continuum of care
3.6.2. Indpendent Variables
(i). Socio-demographic Related Variables
1. Age
2. Religion
3. Ethnicity
4. Educational status
5. Marital statues
6. Occupation
7. Husband age
8. Husband occupation
9. Husbands educational statues
10. Household average income
(ii). Socio Cultural Related Variables
1. Mothers attitude towards continuum of care
2. Exposure to media
3. Getting permission from work
(iii). Obstetric /Reproductive Health Related Variables
1. Number of pregnancy
2. Number of children
3. Was the pregnancy was wanted/planned
(iv). Maternity Care Service Related Variables
1. The time when she start ANC
2. Number of ANC
3. The place of delivery
4. PNC visit
(v). Health Care Service Related Variables
1. Distance to health facility
2. Health facility type (public/privet)
3.7. Operational Definition
1. Maternity continuum of care; The health care services that a woman receives during pregnancy, childbirth, and the immediate postnatal period
| [4] | Akinyemi JO, Afolabi RF, Awolude OA. Patterns and determinants of dropout from maternity care continuum in Nigeria. BMC pregnancy and childbirth. 2016; 16(1): 282. |
| [18] | Tamang TM. Factors Associated with Completion of Continuum of Care for Maternal Health in Nepal. |
[4, 18]
.
2. Drop out from maternity continuum of care: In this study dropout from maternity continuum of care is considered as among women’s who received at least one ANC visit but, did not receive skilled delivery assistants and from those who got skilled birth attendants, did not receive at least one PNC visit within the first 6 week postnatal period in addition to the first 24 hr after institutional delivery
| [4] | Akinyemi JO, Afolabi RF, Awolude OA. Patterns and determinants of dropout from maternity care continuum in Nigeria. BMC pregnancy and childbirth. 2016; 16(1): 282. |
| [5] | Tamang TM, editor Factors associated with completion of continuum of Care for Maternal Health in Nepal. proceedings of the IUSSP XXVIII International Population Conference, Cape Town, South Africa; 2017. |
| [15] | Muluneh AG, Kassa GM, Alemayehu GA, Merid MW. High dropout rate from maternity continuum of care after antenatal care booking and its associated factors among reproductive age women in Ethiopia, Evidence from Demographic and Health Survey 2016. PloS one. 2020; 15(6): e0234741. |
[4, 5, 15]
.
3. Antenatal care; is care in which a woman receives health care service at least one visit from health care providers during her pregnancy.
4. Delivery care; Child birth managed by skilled birth attendants.
5. Skilled birth attendants; An accredited health professional such as a midwife, doctor or nurse who has been educated and trained to proficiency in the skills needed to manage normal (uncomplicated) pregnancies, childbirth and the immediate postnatal period, and in the identification, management and referral of complications in women and newborns.
6. Postnatal care; the care which is given to women and newborn for the first six weeks after childbirth.
3.8. Data Collection Tools and Procedures
The questionnaire was developed after reviewing relevant literatures and modified accordingly. The data was collected using pretested, semi structured and an interviewer- administered questionnaire. It was prepared originally in English and translated into local language Tigrigna for the purpose of data collection to make easy and understandable. For each kebeles, two diploma Midwifery and one heath extension workers for data collection and 1 BSc Midwife for supervisor, total of 9 data collectors and 3 supervisors were recruited for data collection.
3.9. Data Quality Control
The questionnaire was prepared in English, and then translated to Tigrigna (local language) and back to English to maintain consistency of the tool. Before the actual data collection one day training was given for data collectors and supervisors. The data was checked daily for completeness and accuracy by principal investigator, co- investigators and supervisors. Pretest was conducted on (5%) of the sample size out of the study area in Wukro town to ensure the validity, reliability, and clarity of the data collection instrument. Cron batch alpha was used to cheek reliability of the tool. Finally; at the end of the pretest according the result some modification was under taken.
3.10. Data Processing and Analysis
Data cleaning was performed to check for accuracy, completeness, consistencies and missing values and outliers. After the data has checked for completeness and accuracy, it was coded and entered to Epi data version 4.4.4.1 and exported to Statistical Package of Social Science (SPSS) version 22 for statistical analysis. Descriptive analysis was performed using mean, standard deviation, frequencies, proportion to describe study population in relation to dependent and independent variables. Bivariable and multivariable logistic regression model was fitted to identify association between dependent and independent variables. Binary logistic regression was used to identify relation of each independent variable with dependent variables. Variables having p-value less than 0.2 in binary logistic regression were entered to multivariable logistic regression using back ward conditional method for further analysis and to adjust the effect of confounding variables. In multivariable analysis adjusted odds ratio with 95% confidence interval (CI) was used to determine the strength and direction of the association between independent and dependent variable. Model fitness was checked using Hosmer and Lemshow goodness -of -fit, and a p-value >0.05 with 95% confidence interval (CI) was considered as good fitted model.
4. Ethical Considerations
Ethical clearance was obtained from the Institutional Review Board (IRB) of Adigrat University on the behalf of the Ethical Review Committee of collage of Medicine and Health science. A letter of cooperation was obtained from Adigrat town health office. Verbal and written informed consent was obtained from each study participants after explanation of the purpose of the study. Any mother who were not willing to participate in the study was not forced to participate, no personal identifications was included in the data sheet, withdrawal from the study was possible at any time and all data taken from the participants was kept strictly confidential and used only for the study purpose.
5. Results
5.1. Socio-demographic Characteristics of the Respondents
In this study, a total of 357 mothers who gave birth in the last 12 months were interviewed with a response rate of 98.9%. The median age of the respondents was 28 years ± 6 IQR and the median age of their child was 6 months ±4 IQR. Majority (85.4%) of respondents were married out of them 150 (42%) of their husband's occupation were private emploee and 105 (24.9%) of their husband's educational status were collage and above. One hundred seventy four (48.7%) of mothers were secondary education. From 357 study participants (67.5%) of the Mothers occupation were house wife. Only 69 (19.3%) of respondents were household heads. Almost all respondents (88.2%) were orthodox religious followers and 339 (95%) Tigrignan by ethnicity (
Table 1).
Table 1. Socio-demographic characteristics of mothers who gave birth in the last oneyears in Adigrat Town, Eastern Tigray zone, Northern Ethiopia, 2024 (n=361).
Variable | Category | Frequency (n) | Percent (%) |
Religion | Orthodox | 315 | 88.2 |
Muslim | 13 | 3.6 |
Catholic | 29 | 8.1 |
Age of respondent | ≤20 | 44 | 12.3 |
21-34 | 262 | 73.4 |
≥35 | 51 | 14.3 |
Age of child | 0-3 months | 150 | 42 |
4-6 montha months | 76 | 21.3 |
7-12 months | 131 | 36.7 |
Family size | ≤3 | 316 | 88.5 |
≥4 | 41 | 11.5 |
Age of husband | 20-29 | 50 | 16.5 |
30-39 | 193 | 63.5 |
40-49 | 56 | 18.4 |
≥50 | 5 | 1.6 |
Marital status of the mothers | Single | 40 | 11.2 |
Married | 305 | 85.4 |
Widowed | 6 | 1.7 |
Separated | 1 | 0.3 |
Divorced | 5 | 1.4 |
Educational status of husband (n=305) | Unable to write and read | 12 | 3.9 |
Primary school | 91 | 29.9 |
Secondary school | 97 | 31.8 |
Collage and above | 105 | 34.4 |
Occupational status of husband (n=305) | Farmer | 8 | 2.6 |
Merchant | 46 | 15.1 |
Governmental employee | 40 | 13.1 |
Private employee | 150 | 49.1 |
Daily laborer | 20 | 6.5 |
Students | 1 | 0.3 |
Others | 40 | 13.3 |
Occupational status of mother | Housewife | 241 | 67.5 |
Merchant | 18 | 5 |
Private employee | 27 | 7.6 |
Governmental employee | 41 | 11.5 |
Farmer | 2 | 0.6 |
Daily laborer | 2 | 0.6 |
Student | 26 | 7.3 |
Educational status of mother | Unable to read and write | 16 | 4.5 |
Primary school (1-8) | 84 | 23.5 |
Secondary school (9-12) | 174 | 48.7 |
Collage and above | 83 | 23.3 |
Access to mass media | Yes | 231 | 64.7 |
No | 126 | 35.3 |
Household head | Yes | 69 | 19.3 |
No | 288 | 80.7 |
Family wealth index | Low | 52 | 14.6 |
Medium | 29 | 8.1 |
High | 276 | 77.3 |
5.2. Socio-cultural Related Characteristics of the Study Participants
Among respondents, one hundred seventy four (48.7%) of the mothers and new born children get service/treatment from a place other than health institutions, and out of those 109 were got services from traditional healers during pregnancy. Majority of respondents (66.3%) had bad attitude on maternal health care service.
Figure 1. Attitude of mothers who gave birth in the last 12 months in Adigrat town, Northern Ethiopia 2024.
5.3. Reproductive/Obstetrics and Maternity Health Care Service Related Variables
5.3.1. Reproductive/Obstetrics Related Characteristics
Majority of study participants, 152 (42.6%) there pregnancy was for the second time, whereas, 41 (11.5%) of the women had four and more pregnancies. More than half (65.8%) of the respondents their last pregnancy was planned, and more than 3/4
th (85.4%) of the respondents' last pregnancy was wanted. One hundred eight (30.3%) of mothers had only one child, and 33 (12.3%) of mothers had four and more children (
Table 2).
Table 2. Reproductive/obstetrics related characteristics of mothers who gave birth in the last one years in Adigrat Town, Eastern Tigray zone, Northern Ethiopia, 2024 (n=361).
Variable | Category | Frequency (n) | Percent (%) |
Number of pregnancy | 1 | 104 | 29.1 |
2 | 152 | 42.6 |
3 | 60 | 16.8 |
≥ 4 | 41 | 11.5 |
Was the pregnancy planned | Yes | 235 | 65.8 |
No | 122 | 34.2 |
Was the pregnancy wanted | Yes | 305 | 85.4 |
No | 52 | 14.6 |
Number of alive children | 1 | 108 | 30.3 |
2 | 142 | 39.8 |
3 | 63 | 17.6 |
≥ 4 | 33 | 12.3 |
Abortion history | Yes | 237 | 66.4 |
No | 120 | 33.6 |
Service satisfaction | very satisfied | 38 | 10.6 |
Satisfied | 202 | 56.6 |
Very dissatisfied | 81 | 22.7 |
Dis satisfied | 36 | 10.1 |
5.3.2. Maternal Health Care Service Utilization Related Characteristics of Respondents
Around 2/3rd of mothers (66.4%) never heard about maternal health care services. More than half (50.4%) of the study participant’s start their first antenatal care follow up at 4-7 months of pregnancy. More than one third of 119 (33.3%) of the women their ANC follow up were at public hospitals. Among respondents, 130 (36.4%) of the women had four and more times ANC follow up during their recent pregnancy. Among the study participants, 254 (71.1%) were gave birth their last baby at the public hospital, and twenty (5.6%) of the respondents delivered their last baby at home. More than half of study participants 214 (59.9/%) were did not get available transportation to health facility (
Table 3).
Table 3. Maternal health care service utilization related characteristics of respondents mothers who gave birth in the last one years in Adigrat Town, Eastern Tigray zone, Northern Ethiopia, 2024 (n=361).
Variable | Category | Frequency (n) | Percent (%) |
Mother ever heard about health care service | Yes | 120 | 33.6 |
No | 237 | 66.4 |
Husband ever heard on maternal health care service (n=305) | Yes | 244 | 80 |
No | 61 | 20 |
About what health care service (n=262) | ANC | 63 | 24.1 |
ANC and DC | 1 | 0.4 |
ANC, DC and PNC | 198 | 75.5 |
Number of ANC visit | <4 visit | 227 | 63.6 |
≥ 4 | 130 | 36.4 |
Months of pregnancy at first visit (n=357) | 1-3 months | 177 | 49.6 |
4-7 months | 180 | 50.4 |
Place of ANC (n=357) | Heath center | 100 | 28 |
Private hospital | 89 | 24.9 |
Public hospital | 119 | 33.3 |
HC and PH | 2 | 0.6 |
HC, PH and PI | 1 | 0.3 |
HC and private | 5 | 1.4 |
PH and private | 41 | 11.5 |
Time spent of ANC visit | <15 minutes | 128 | 35.9 |
≥15 minutes | 229 | 64.1 |
Place of last baby delivery (n=357) | Health center | 58 | 16.2 |
Public hospital | 254 | 71.2 |
Private | 25 | 7 |
Home | 20 | 5.6 |
PNC visit (n=357) | Yes | 148 | 41.5 |
No | 209 | 58.5 |
Available transportation | Yes | 214 | 59.9 |
no | 143 | 40.1 |
Internally displaced | Yes | 32 | 9 |
No | 325 | 91 |
Distance to health facility | 0.5 -4km | 354 | 99.2 |
≥ 5km | 3 | 0.8 |
Permission from work place | Yes | 224 | 62.7 |
No | 133 | 37.3 |
Health care provider support | Yes | 234 | 65.5 |
No | 123 | 34.5 |
ANC counseling on MCC | Yes | 239 | 66.9 |
No | 118 | 33.1 |
5.4. Proportion of Drop Outs from Maternity Continuum of Care
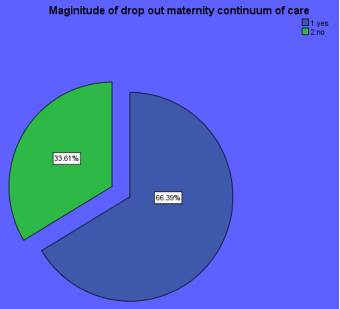
The overall magnitude of drop out from the maternity continuum of care was 237 (66.4%) [95%CI (61.3-70.9)]. In addition to this in this study 200 (60.6%) of respondents had less than four ANC visit, 20 (5.6%) also drop out from skill birth attendant and 209 (58.9%) of them had no postnatal follow up after meeting with skill birth attendant.
Figure 2. Drop out from maternity continuum of care mothers who gave birth in the last one years in Adigrat Town, Eastern Tigray zone, Northern Ethiopia, 2024 (n=361).
5.5. Factors Associated with Drop out from Maternity Continuum of Care
Variables having p-value of less than 0.2 in the bivariable analysis were considered as significant variables so that, they were included into the multivariable analysis, household head, mother ever heard on maternal health care service, heath care service out of health facility, exposure to mass media, wanted pregnancy, planned pregnancy, number of ANC visit, permission from work, availability of transportation, abortion history and attitude were statistically significant factors associated with drop out from maternity continuum of care in multivariable logistic regression analysis. After adjusting the effect of confounding variables, mother ever heard on maternal health care service, health service out of health facility, abortion history, planned pregnancy, number of ANC and attitude of mother to maternal health care service were statistically significant factors associated with drop out from maternity continuum of care in multivariable logistic regression analysis. Mothers never heard on maternal health care service were 4.2 times more likely to drop out from maternity continuum of care (AOR=4.179 (1.107, 15.783) as compared to their counterparts. Respondents who get service out of health facility were 5 times higher dropout rate (AOR 5.136 (1.988, 13.267) relative to mothers did not get health service out of health facility. Mothers who had no abortion history were 1.4 times more likely to drop out from maternity continuum of care AOR=1.424 (1.113, 12.133) as compared to mother who had abortion. Those mothers whose pregnancy was un planned were 5.5 times more likely to drop out from maternity continuum of care as AOR=5.478 (1.902, 15.777) compared to those mothers who had planned pregnancy. Respondents who had less than 4 ANC were 5.5 more likely to dropout from maternity continuum of care (AOR= 5.583 (2.598, 11. 997) as compared to mothers who had more than or equals to 4 ANC visit. In addition, the odds of drop out from maternity continuum of was 15 times higher in mothers who had bad attitude (AOR=15.049 (2.489, 32.997) as compared to their counter parts (
Table 4).
Table 4. Bivariable and multivariable logistic regression analysis showing factors associated with drop out from maternity continuum of care mothers who gave birth in the last one years in Adigrat Town, Eastern Tigray zone, Northern Ethiopia, 2024 (n=361).
Variables | Drop out | COR (95% CI) | AOR (95%CI) |
Yes | no |
House hold head | | | | |
Yes | 55 | 14 | 2.28 (1.23, 3.45) | 0.283 (0.121, 0.66) |
No | 182 | 106 | 1 |
Mother ever heard on maternal health care service |
Yes | 109 | 11 | 1 | 1 |
No | 153 | 84 | 5.44 (2.771, 10.682) | 4.179 (1.107, 15.783)* |
Health service out of health facility | | | | |
Yes | 147 | 27 | 5.62 (3.541, 12.601) | 5.136 (1.988, 13.267)** |
No | 90 | 93 | 1 | 1 |
Exposure to mass media | | | | |
Yes | 89 | 142 | 1 | 1 |
No | 31 | 95 | 1.921 (1.183, 3.18) | 0.268 (0.121, 0.661) |
Abortion history | | | | |
Yes | 205 | 32 | 1 | 1 |
No | 96 | 24 | 1.601 (1.962, 8.342) | 1.424 (1.113, 12.133) |
Planned pregnancy | | | | |
Yes | 112 | 123 | 1 | 1 |
No | 8 | 114 | 13.468 (8.234, 22.567) | 5.478 (1.902, 15.777)* |
Wanted pregnancy | | | | |
Yes | 216 | 89 | 1 | 1 |
No | | 37 | 5.986 (16.52, 45.342) | 3.321 (1.381, 10.579) |
Available transportation | 15 | | | |
Yes | 169 | 45 | 1 | 1 |
No | 68 | 75 | 4.142 (2.345, 6.890) | 2.019, 1.031, 3.954) |
Number of ANC | | | | |
<4 | 180 | 47 | 6.542 (3.837, 13.409) | 1 |
≥ 4 | 48 | 82 | 1 | 5.583 (2.598, 11.997)** |
Attitude | | | | |
Good | 118 | 2 | 1 | 1 |
Bad | 168 | 69 | 24.232 (16, 201, 45.678) | 15.049 (2.489, 32.997)* |
Permission from work | | | | |
Yes | 213 | 11 | 1 | 1 |
No | 101 | 32 | 6.129 (0.795, 47.773) | 4.831 (0.533, 34.811) |
NB: *=P<0.05 **=P<0.001 1 Reference Hosmer and lemshow goodness -of- fit p- value=0.644 COR =Crude odds ratio, AOR=Adjusted Odds Ratio CI=Confidence interval
6. Discussion
Drop out from maternity conitunuum of care is public health problem in world wide as well as in ethiopia. In this study the over all prevalance of drop out from maternity conittunm of care was found high which was 237 (66.4%) [95%CI (61.3-70.9)]. This finding (66.4%) is higher than the studies conducted in Nigeria (38.1%), Tanzania (10%) Nepal (50%) Northwest Ethiopian and Addis Abeba [58.39%] (32.2%)
| [11] | Mohan D, LeFevre AE, George A, Mpembeni R, Bazant E, Rusibamayila N, et al. Analysis of dropout across the continuum of maternal health care in Tanzania: findings from a cross-sectional household survey. Health policy and planning. 2017; 32(6): 791-9. |
| [19] | Akinyemi JO, Afolabi RF, Awolude OA. Patterns and determinants of dropout from maternity care continuum in Nigeria. BMC pregnancy and childbirth. 2016; 16: 1-11. |
| [20] | Tamang TM, editor Factors associated with completion of continuum of Care for Maternal Health in Nepal. IUSSP XXVIII International Population Conference, Cape Town, South Africa; 2017. |
| [21] | Amare NS, Araya BM, Asaye MM. The proportion of dropouts from the maternity continuum of care and its predictors among antenatal booked women who gave birth in the last 12 months in Northwest Ethiopian women: a community-based cross-sectional study. Pan African Medical Journal. 2022; 41(1). |
| [22] | Desta DZ, Kebede A, Merid MW, Negash WD, Asmamaw DB. The dropout rate and associated factors of the continuum of maternal health care services before and during Covid-19 Pandemic among women who gave birth in the last two years in Addis Ababa, Ethiopia, 2021. A comparative cross-sectional study design. 2021. |
[11, 19-22]
. This discrepancy may be due to sociocultural difference, awareness on maternal health care service, access to health care service and study area and sample size varation.
This finding is also consistent with studies conducted in Debre Brhan town (69.1%), Northwest Ethiopia [63.4%]
| [17] | Tadese M, Tessema SD, Aklilu D, Wake GE, Mulu GB. Dropout from a maternal and newborn continuum of care after antenatal care booking and its associated factors in Debre Berhan town, northeast Ethiopia. Frontiers in Medicine. 2022; 9: 950901. |
| [23] | Tsega D, Admas M, Talie A, Tsega TB, Birhanu MY, Alemu S, et al. Maternity continuum care completion and its associated factors in Northwest Ethiopia. Journal of Pregnancy. 2022. |
[17, 23]
. This similarity might be due to they have similar socio-cultural practices and both Adigrat and DebreBrhane founds in northern part of Ethiopia and in both there was war and they may affect the maternal health care service.
However, it is lower than the national prevalence of drop out from maternity continuum of care [93.4%], AribaMinche Zuria [90.3%], Chelia district [88.5%], west Gojjam Zone [87.9%] from Tanzania Demographic Health Survey [83.86%],
| [15] | Muluneh AG, Kassa GM, Alemayehu GA, Merid MW. High dropout rate from maternity continuum of care after antenatal care booking and its associated factors among reproductive age women in Ethiopia, Evidence from Demographic and Health Survey 2016. PloS one. 2020; 15(6): e0234741. |
| [22] | Desta DZ, Kebede A, Merid MW, Negash WD, Asmamaw DB. The dropout rate and associated factors of the continuum of maternal health care services before and during Covid-19 Pandemic among women who gave birth in the last two years in Addis Ababa, Ethiopia, 2021. A comparative cross-sectional study design. 2021. |
| [24] | Asnake AA, Abajobir AA, Seifu BL, Asgedom YS, Melese M, Bezie MM, et al. Multilevel analysis of dropout from maternal continuum of care and its associated factors: Evidence from 2022 Tanzania Demographic and Health Survey. Plos one. 2024; 19(5): e0302966. |
| [25] | Haile D, Kondale M, Andarge E, Tunje A, Fikadu T, Boti N. Level of completion along continuum of care for maternal and newborn health services and factors associated with it among women in Arba Minch Zuria woreda, Gamo zone, Southern Ethiopia: A community based cross-sectional study. Plos one. 2020; 15(6): e0221670. |
| [26] | Buli TD, Wakgari N, Ganfure G, Wondimu F, Dube DL, Moti G, et al. Completion of the continuum of maternity care and associated factors among women who gave birth in the last 6 months in Chelia district, West Shoa zone, Ethiopia: A community-based cross-sectional study. Frontiers in Public Health. 2023; 10: 1026236. |
| [27] | Emiru AA, Alene GD, Debelew GT. Women’s retention on the continuum of maternal care pathway in west Gojjam zone, Ethiopia: multilevel analysis. BMC pregnancy and childbirth. 2020; 20: 1-14. |
[15, 22, 24-27]
. The difference might be due to socio-demographic, educational status and cultural variability and year of study. This two to three years variation of may bring awareness differences about maternal health care service and health-seeking behavior of the community.
Concerning factors associated with drop out maternity continuum of care mothers never heard on maternal health care service were 4.2 times more likely to drop out from maternity continuum of care (AOR=4.179 (1.107, 15.783) as compared to their counterparts. The possible explanation might be due to the fact that mothers who heard on maternal health care serve may have good knowledge on the advantage of maternal health care service in redaction of maternal and neonatal mortality and may have good health seeking behavior than mothers never heard on maternal health care service
| [21] | Amare NS, Araya BM, Asaye MM. The proportion of dropouts from the maternity continuum of care and its predictors among antenatal booked women who gave birth in the last 12 months in Northwest Ethiopian women: a community-based cross-sectional study. Pan African Medical Journal. 2022; 41(1). |
| [28] | Abebe GF, Belachew DZ, Girma D, Aydiko A, Negesse Y. Multilevel analysis of the predictors of completion of the continuum of maternity care in Ethiopia; using the recent 2019 Ethiopia mini demographic and health survey. BMC Pregnancy and Childbirth. 2022; 22(1): 691. |
[21, 28]
.
This study also indicated that respondents who get service out of health facility were 5 times higher dropout rate (AOR =5.136 (1.988, 13.267) relative to mothers did not get health service out of health facility. One potential explanation could be that moms receiving care outside of a medical facility lack awareness of the risks associated with traditional practices, which are mostly influenced by their grandparents.
Furthermore, mothers whose pregnancy was un planned were 5.5 times more likely to drop out from maternity continuum of care as AOR=5.478 (1.902, 15.777) compared to those mothers who had planned pregnancy. This result is supported by study done in North West Ethiopia, AribaMinche Zuria, and Chelia district
| [21] | Amare NS, Araya BM, Asaye MM. The proportion of dropouts from the maternity continuum of care and its predictors among antenatal booked women who gave birth in the last 12 months in Northwest Ethiopian women: a community-based cross-sectional study. Pan African Medical Journal. 2022; 41(1). |
| [25] | Haile D, Kondale M, Andarge E, Tunje A, Fikadu T, Boti N. Level of completion along continuum of care for maternal and newborn health services and factors associated with it among women in Arba Minch Zuria woreda, Gamo zone, Southern Ethiopia: A community based cross-sectional study. Plos one. 2020; 15(6): e0221670. |
| [26] | Buli TD, Wakgari N, Ganfure G, Wondimu F, Dube DL, Moti G, et al. Completion of the continuum of maternity care and associated factors among women who gave birth in the last 6 months in Chelia district, West Shoa zone, Ethiopia: A community-based cross-sectional study. Frontiers in Public Health. 2023; 10: 1026236. |
[21, 25, 26]
. A possible explanation for the correlation between MCC and intended pregnancy is that early pregnancy planning would decrease ANC delays, perhaps increasing the likelihood of many visits along the MCC
| [29] | Ewunetie AA, Munea AM, Meselu BT, Simeneh MM, Meteku BT. DELAY on first antenatal care visit and its associated factors among pregnant women in public health facilities of Debre Markos town, North West Ethiopia. BMC pregnancy and childbirth. 2018; 18: 1-8. |
| [30] | Mose A, Haile K, Timerga A. Prevalence of completion of maternity continuum of care and its associated factors in Ethiopia: a systematic review and meta-analysis. BMJ open. 2022; 12(11): e062461. |
| [31] | Mengistie HT, Belay MA, Sendekie AD, Shitie A, Sewyew DA. Complete continuum of maternity care and associated factors among mothers who gave birth in the last twelve months in Mekane Selam town North-East Ethiopia: A community-based cross-sectional study, 2021. Plos one. 2023; 18(9): e0289200. |
[29-31]
.
Compared to mothers who had abortion history, mothers who had no prior abortions had 1.4-fold increased risk of dropping out of the maternity continuum (AOR=1.424 (1.113, 12.133). This might be due to the fact that the past bad history of pregnancy making them to focus carefully on the present pregnancy outcome
| [31] | Mengistie HT, Belay MA, Sendekie AD, Shitie A, Sewyew DA. Complete continuum of maternity care and associated factors among mothers who gave birth in the last twelve months in Mekane Selam town North-East Ethiopia: A community-based cross-sectional study, 2021. Plos one. 2023; 18(9): e0289200. |
| [32] | Hunie Asratie M, Belay DG. Pooled prevalence and determinants of completion of maternity continuum of care in Sub-Saharan Africa: a multi-country analysis of recent demographic and health surveys. Frontiers in Global Women's Health. 2022; 3: 869552. |
[31, 32]
and the effort of health care providers intervention with bad obstetrics history might increase the health seeking behaviors
| [33] | Suryanarayana R, Chandrappa M, Santhuram AN, Prathima S, Sheela S. Prospective study on prevalence of anemia of pregnant women and its outcome: A community based study. Journal of family medicine and primary care. 2017; 6(4): 739-43. |
[33]
this might be help to achieve MCC with mothers had abortion history.
In this study, respondents who had less than 4 ANC were 5.5 more likely to dropout from maternity continuum of care (AOR= 5.583 (2.598, 11. 997) as compared to mothers who had more than or equals to 4 ANC visit. This conclusion may be explained by the fact that early initiation of ANC provides a good chance for mothers to get a good health promotion and to learn about pregnancy danger signs and obstetric risks in early time and this will improve health seeking behaviors of the mothers
| [30] | Mose A, Haile K, Timerga A. Prevalence of completion of maternity continuum of care and its associated factors in Ethiopia: a systematic review and meta-analysis. BMJ open. 2022; 12(11): e062461. |
| [31] | Mengistie HT, Belay MA, Sendekie AD, Shitie A, Sewyew DA. Complete continuum of maternity care and associated factors among mothers who gave birth in the last twelve months in Mekane Selam town North-East Ethiopia: A community-based cross-sectional study, 2021. Plos one. 2023; 18(9): e0289200. |
| [34] | Yaya S, Bishwajit G, Ekholuenetale M, Shah V, Kadio B, Udenigwe O. Timing and adequate attendance of antenatal care visits among women in Ethiopia. PloS one. 2017; 12(9): e0184934. |
[30, 31, 34]
.
In addition, the odds of drop out from maternity continuum of was 15 times higher in mothers who had bad attitude (AOR=15.049 (2.489, 32.997) as compared to their counter parts. The explanation could be that mothers who have a positive attitude toward maternal health care services may begin early antenatal care and have the opportunity to discuss the significance of the maternity continuum of care in reducing maternal and infant mortality with their healthcare provider.
7. Strength and Limitations of the Study
7.1. Strength of the Study
It is community based study it takes more resources.
Family wealth index was computed by using PCA.
7.2. Limitations of the Study
It could be prone to recall base since data were taken from the mothers backward history.
This study is not supported by qualitative study to dig out the cultural belief of the community.
8. Conclusion
This study revealed that drop out from maternity continuum of care was high as compared to WHO recommendations. Mothers ever heard on maternal health care service, planned pregnancy, number of ANC visit, mothers attitude, abortion history and health service out of health facility were statically significant independent factors associated with drop out from maternity continuum of care.
Abbreviations
ANC | Antenatal Care |
AOR | Adjested Odds Ratio |
COR | Curde Odds Ratio |
EDHS | Ethiopian Demographic Health Servey |
HC | Health Center |
HI | Hospital |
MCC | Maternity Contunnm of Care |
PCA | Principal Compenent Anlaysis |
PNC | Post Natal Care |
SPSS | Stastical package for Social Science |
WHO | World Health Organazation |
Availability of Data and Materials
The corresponding author might seek access to the datasets used to support the results in this article.
Authors’ Contributions
MG and WM were involved in the study's inception and design, while MG, WM and KMW were responsible for data interpretation and the first draft of the publication. In commenting on the document, NSK and MG took part. Each author reviewed the completed work critically and gave their approval after reading it.
Ethics Approval and Consent to Participate
The Institutional Review Board at Adigrat University provided ethical clearance and approval. After then, a formal letter was sent to the local health office of Adigrat. Participants gave their verbal informed permission after being fully aware of the study's goal and aim. At every stage of the research, confidentiality was upheld. Participants were asked to participate in the study voluntarily, and those who wished to withdraw from it were given full permission to do so.
Consent for Publication
Not applicable.
Funding
Author(s) have not received any specific funding for this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Owili PO, Muga MA, Mendez BR, Chen B. Quality of maternity care and its determinants along the continuum in Kenya: A structural equation modeling analysis. PloS one. 2017; 12(5): e0177756.
|
| [2] |
Kerber KJ, de Graft-Johnson JE, Bhutta ZA, Okong P, Starrs A, Lawn JE. Continuum of care for maternal, newborn, and child health: from slogan to service delivery. The Lancet. 2007; 370(9595): 1358-69.
|
| [3] |
Agarwal S, Curtis S, Angeles G, Speizer I, Singh K, Thomas J. Are community health workers effective in retaining women in the maternity care continuum? Evidence from India. BMJ Global Health. 2019; 4(4): e001557.
|
| [4] |
Akinyemi JO, Afolabi RF, Awolude OA. Patterns and determinants of dropout from maternity care continuum in Nigeria. BMC pregnancy and childbirth. 2016; 16(1): 282.
|
| [5] |
Tamang TM, editor Factors associated with completion of continuum of Care for Maternal Health in Nepal. proceedings of the IUSSP XXVIII International Population Conference, Cape Town, South Africa; 2017.
|
| [6] |
Organization WH. World health statistics 2015: World Health Organization; 2015.
|
| [7] |
Alkema L, Chou D, Hogan D, Zhang S, Moller A-B, Gemmill A, et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. The Lancet. 2016; 387(10017): 462-74.
|
| [8] |
Singh K, Story WT, Moran AC. Assessing the continuum of care pathway for maternal health in South Asia and sub-Saharan Africa. Maternal and child health journal. 2016; 20(2): 281-9.
|
| [9] |
Anastasi E, Borchert M, Campbell OM, Sondorp E, Kaducu F, Hill O, et al. Losing women along the path to safe motherhood: why is there such a gap between women’s use of antenatal care and skilled birth attendance? A mixed methods study in northern Uganda. BMC pregnancy and childbirth. 2015; 15(1): 287.
|
| [10] |
Landers C. Maternal and newborn health: a global challenge. The State of the World's Children New York, NY: United Nations Children's Fund. 2009; 5.
|
| [11] |
Mohan D, LeFevre AE, George A, Mpembeni R, Bazant E, Rusibamayila N, et al. Analysis of dropout across the continuum of maternal health care in Tanzania: findings from a cross-sectional household survey. Health policy and planning. 2017; 32(6): 791-9.
|
| [12] |
Wang W. Levels and trends in the use of maternal health services in developing countries: ICF Macro; 2011.
|
| [13] |
Kikuchi K, Yasuoka J, Nanishi K, Ahmed A, Nohara Y, Nishikitani M, et al. Postnatal care could be the key to improving the continuum of care in maternal and child health in Ratanakiri, Cambodia. PloS one. 2018; 13(6): e0198829.
|
| [14] |
Ethiopian Public Health Institute FMoH, Addis Ababa, Ethiopia, and The DHS Program, ICF, Rockville, Maryland, USA. Mini Demographic and Health Survey. 2019.
|
| [15] |
Muluneh AG, Kassa GM, Alemayehu GA, Merid MW. High dropout rate from maternity continuum of care after antenatal care booking and its associated factors among reproductive age women in Ethiopia, Evidence from Demographic and Health Survey 2016. PloS one. 2020; 15(6): e0234741.
|
| [16] |
EMOH. Ethiopia Voluntary National Review on SDGs Government Commitments, National Ownership and Performance Trends. 2017.
|
| [17] |
Tadese M, Tessema SD, Aklilu D, Wake GE, Mulu GB. Dropout from a maternal and newborn continuum of care after antenatal care booking and its associated factors in Debre Berhan town, northeast Ethiopia. Frontiers in Medicine. 2022; 9: 950901.
|
| [18] |
Tamang TM. Factors Associated with Completion of Continuum of Care for Maternal Health in Nepal.
|
| [19] |
Akinyemi JO, Afolabi RF, Awolude OA. Patterns and determinants of dropout from maternity care continuum in Nigeria. BMC pregnancy and childbirth. 2016; 16: 1-11.
|
| [20] |
Tamang TM, editor Factors associated with completion of continuum of Care for Maternal Health in Nepal. IUSSP XXVIII International Population Conference, Cape Town, South Africa; 2017.
|
| [21] |
Amare NS, Araya BM, Asaye MM. The proportion of dropouts from the maternity continuum of care and its predictors among antenatal booked women who gave birth in the last 12 months in Northwest Ethiopian women: a community-based cross-sectional study. Pan African Medical Journal. 2022; 41(1).
|
| [22] |
Desta DZ, Kebede A, Merid MW, Negash WD, Asmamaw DB. The dropout rate and associated factors of the continuum of maternal health care services before and during Covid-19 Pandemic among women who gave birth in the last two years in Addis Ababa, Ethiopia, 2021. A comparative cross-sectional study design. 2021.
|
| [23] |
Tsega D, Admas M, Talie A, Tsega TB, Birhanu MY, Alemu S, et al. Maternity continuum care completion and its associated factors in Northwest Ethiopia. Journal of Pregnancy. 2022.
|
| [24] |
Asnake AA, Abajobir AA, Seifu BL, Asgedom YS, Melese M, Bezie MM, et al. Multilevel analysis of dropout from maternal continuum of care and its associated factors: Evidence from 2022 Tanzania Demographic and Health Survey. Plos one. 2024; 19(5): e0302966.
|
| [25] |
Haile D, Kondale M, Andarge E, Tunje A, Fikadu T, Boti N. Level of completion along continuum of care for maternal and newborn health services and factors associated with it among women in Arba Minch Zuria woreda, Gamo zone, Southern Ethiopia: A community based cross-sectional study. Plos one. 2020; 15(6): e0221670.
|
| [26] |
Buli TD, Wakgari N, Ganfure G, Wondimu F, Dube DL, Moti G, et al. Completion of the continuum of maternity care and associated factors among women who gave birth in the last 6 months in Chelia district, West Shoa zone, Ethiopia: A community-based cross-sectional study. Frontiers in Public Health. 2023; 10: 1026236.
|
| [27] |
Emiru AA, Alene GD, Debelew GT. Women’s retention on the continuum of maternal care pathway in west Gojjam zone, Ethiopia: multilevel analysis. BMC pregnancy and childbirth. 2020; 20: 1-14.
|
| [28] |
Abebe GF, Belachew DZ, Girma D, Aydiko A, Negesse Y. Multilevel analysis of the predictors of completion of the continuum of maternity care in Ethiopia; using the recent 2019 Ethiopia mini demographic and health survey. BMC Pregnancy and Childbirth. 2022; 22(1): 691.
|
| [29] |
Ewunetie AA, Munea AM, Meselu BT, Simeneh MM, Meteku BT. DELAY on first antenatal care visit and its associated factors among pregnant women in public health facilities of Debre Markos town, North West Ethiopia. BMC pregnancy and childbirth. 2018; 18: 1-8.
|
| [30] |
Mose A, Haile K, Timerga A. Prevalence of completion of maternity continuum of care and its associated factors in Ethiopia: a systematic review and meta-analysis. BMJ open. 2022; 12(11): e062461.
|
| [31] |
Mengistie HT, Belay MA, Sendekie AD, Shitie A, Sewyew DA. Complete continuum of maternity care and associated factors among mothers who gave birth in the last twelve months in Mekane Selam town North-East Ethiopia: A community-based cross-sectional study, 2021. Plos one. 2023; 18(9): e0289200.
|
| [32] |
Hunie Asratie M, Belay DG. Pooled prevalence and determinants of completion of maternity continuum of care in Sub-Saharan Africa: a multi-country analysis of recent demographic and health surveys. Frontiers in Global Women's Health. 2022; 3: 869552.
|
| [33] |
Suryanarayana R, Chandrappa M, Santhuram AN, Prathima S, Sheela S. Prospective study on prevalence of anemia of pregnant women and its outcome: A community based study. Journal of family medicine and primary care. 2017; 6(4): 739-43.
|
| [34] |
Yaya S, Bishwajit G, Ekholuenetale M, Shah V, Kadio B, Udenigwe O. Timing and adequate attendance of antenatal care visits among women in Ethiopia. PloS one. 2017; 12(9): e0184934.
|
Cite This Article
-
APA Style
Teka, M. G., Werde, W. M., Kahisay, N. S., Weldeyohans, K. M., Weldegebreal, Z. H. (2024). Dropout from Maternity Continuum of Care and Associated Factors Among Mothers Who Gave Birth After War in Adigrat Town, Tigray, Northern Ethiopia 2024. American Journal of Life Sciences, 12(6), 121-133. https://doi.org/10.11648/j.ajls.20241206.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Teka, M. G.; Werde, W. M.; Kahisay, N. S.; Weldeyohans, K. M.; Weldegebreal, Z. H. Dropout from Maternity Continuum of Care and Associated Factors Among Mothers Who Gave Birth After War in Adigrat Town, Tigray, Northern Ethiopia 2024. Am. J. Life Sci. 2024, 12(6), 121-133. doi: 10.11648/j.ajls.20241206.13
Copy
|
Download
AMA Style
Teka MG, Werde WM, Kahisay NS, Weldeyohans KM, Weldegebreal ZH. Dropout from Maternity Continuum of Care and Associated Factors Among Mothers Who Gave Birth After War in Adigrat Town, Tigray, Northern Ethiopia 2024. Am J Life Sci. 2024;12(6):121-133. doi: 10.11648/j.ajls.20241206.13
Copy
|
Download
-
@article{10.11648/j.ajls.20241206.13,
author = {Maezu Gebreslassie Teka and Weldu Mamo Werde and Niguse Shishay Kahisay and Kiflay Mulugeta Weldeyohans and Znabu Hagos Weldegebreal},
title = {Dropout from Maternity Continuum of Care and Associated Factors Among Mothers Who Gave Birth After War in Adigrat Town, Tigray, Northern Ethiopia 2024
},
journal = {American Journal of Life Sciences},
volume = {12},
number = {6},
pages = {121-133},
doi = {10.11648/j.ajls.20241206.13},
url = {https://doi.org/10.11648/j.ajls.20241206.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajls.20241206.13},
abstract = {Background: Maternity continuum of care is the continuity of maternal health care services given to mothers during antenatal period, child birth and post natal period. It is one of the strategic programs meant to lower the death rates of mothers, newborns, and children. In spite of this, a large number of moms discontinue their participation in maternal continuum care. Dropout from the maternity continuum of care is prevalent public health issue in underdeveloped nations, such as Ethiopia. Methods: Community based quantitative cross-sectional study was carried out among 357 mothers who gave birth in the 12 months in Adigrat town. Systematic sampling method was used to obtain study participants. Data was collected using pretested, semi- structured and face to face interviewer administered questioner. Bivariable and multivariable logistic regression model was fitted. Variables having p-value less than 0.2 in bivariable analysis was entered to multivariable logistic regression model. In multivariable logistic regression adjusted odds ratio with 95% confidence interval was used to determine strength and direction of the association between dependent and independent variables. Results: The overall magnitude of drop out from the maternity continuum of care was 237 (66.4%) [95%CI (61.3-70.9)], 60.6% drop out from ANC visit, 5.6% drop out from skill birth attendant and 58.9% drop out from PNC. Mothers never heard on maternal health care service (AOR=4.179 (1.107, 15.783), service out of health facility (AOR =5.136 (1.988, 13.267) noabortionhistory (AOR=1.424 (1.113, 12.133), unplannedpregnancy (AOR=5.478 (1.902, 15.777), less than 4 ANC visit (AOR= 5.583 (2.598, 11. 997) and mothers attitude (AOR=15.049 (2.489, 32.997) were statically significant factors associated with drop out from maternity continuum of care. Conclusion and discussion: This study showed that magnitude of drop out from maternity continuum of care was high as compared to WHO recommendations. As a result concerned stakeholders and policy makers should initiate more than four ANC visit, create awareness on harmful traditional practice, bad pregnancy history, support mothers to use family planning to prevent unplanned pregnancy, and work on attitude change of the community.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Dropout from Maternity Continuum of Care and Associated Factors Among Mothers Who Gave Birth After War in Adigrat Town, Tigray, Northern Ethiopia 2024
AU - Maezu Gebreslassie Teka
AU - Weldu Mamo Werde
AU - Niguse Shishay Kahisay
AU - Kiflay Mulugeta Weldeyohans
AU - Znabu Hagos Weldegebreal
Y1 - 2024/11/12
PY - 2024
N1 - https://doi.org/10.11648/j.ajls.20241206.13
DO - 10.11648/j.ajls.20241206.13
T2 - American Journal of Life Sciences
JF - American Journal of Life Sciences
JO - American Journal of Life Sciences
SP - 121
EP - 133
PB - Science Publishing Group
SN - 2328-5737
UR - https://doi.org/10.11648/j.ajls.20241206.13
AB - Background: Maternity continuum of care is the continuity of maternal health care services given to mothers during antenatal period, child birth and post natal period. It is one of the strategic programs meant to lower the death rates of mothers, newborns, and children. In spite of this, a large number of moms discontinue their participation in maternal continuum care. Dropout from the maternity continuum of care is prevalent public health issue in underdeveloped nations, such as Ethiopia. Methods: Community based quantitative cross-sectional study was carried out among 357 mothers who gave birth in the 12 months in Adigrat town. Systematic sampling method was used to obtain study participants. Data was collected using pretested, semi- structured and face to face interviewer administered questioner. Bivariable and multivariable logistic regression model was fitted. Variables having p-value less than 0.2 in bivariable analysis was entered to multivariable logistic regression model. In multivariable logistic regression adjusted odds ratio with 95% confidence interval was used to determine strength and direction of the association between dependent and independent variables. Results: The overall magnitude of drop out from the maternity continuum of care was 237 (66.4%) [95%CI (61.3-70.9)], 60.6% drop out from ANC visit, 5.6% drop out from skill birth attendant and 58.9% drop out from PNC. Mothers never heard on maternal health care service (AOR=4.179 (1.107, 15.783), service out of health facility (AOR =5.136 (1.988, 13.267) noabortionhistory (AOR=1.424 (1.113, 12.133), unplannedpregnancy (AOR=5.478 (1.902, 15.777), less than 4 ANC visit (AOR= 5.583 (2.598, 11. 997) and mothers attitude (AOR=15.049 (2.489, 32.997) were statically significant factors associated with drop out from maternity continuum of care. Conclusion and discussion: This study showed that magnitude of drop out from maternity continuum of care was high as compared to WHO recommendations. As a result concerned stakeholders and policy makers should initiate more than four ANC visit, create awareness on harmful traditional practice, bad pregnancy history, support mothers to use family planning to prevent unplanned pregnancy, and work on attitude change of the community.
VL - 12
IS - 6
ER -
Copy
|
Download